

The news headlines about mutated COVID strains originating in the UK, South Africa, and elsewhere have spread anxiety about the implications for organizations and individuals alike. Recently identified in the US, these strains likely arrived here by mid-November, with hundreds of probable cases by now. Yet should you be truly worried and change your plans?
The media, experts, and officials have focused on concerns about vaccine effectiveness. While some legitimate concerns exist that our vaccines might be 10-20% less effective against the new strains, this relatively small difference shouldn’t make you too worried. In fact, scientists may quickly update the mRNA-based vaccines from Moderna and Pfizer/BioNTech to make them fully effective against these new COVID variants.
So once the US achieves herd immunity through mass vaccination by the end of 2021, these new strains won’t really matter. However, another aspect of these new strains should make you very worried indeed: they’re much more infectious.
Unfortunately, the implications of their infectiousness have received little news coverage. Moreover, prominent public officials have downplayed concerns about the new strain, saying there’s no cause for alarm. For example, Adm. Brett Giroir, the White House coronavirus testing czar, gave an interview on December 27 to “Fox News Sunday,” where he said “It is not any more serious than the normal stains of COVID.”
Such complacency reflects our sleepwalking in the pandemic’s early stages, despite numerous warnings from myself and other risk management experts. Our brains don’t deal well with such threats, making it much more difficult to adapt successfully to slow-moving and high-impact train wrecks such as the pandemic itself, or to a much more infectious variant.
Are the New Strains Really More Infectious?
Research shows that the UK strain is anywhere from 56% to 70% more infectious, meaning each individual person who gets the new strain infects 56-70% more people than the older COVID strain. The new variant quickly came to dominate the old strain of COVID in Southeast England, going from less than 1% of all tested samples at the start of November to over two-thirds by mid-December.
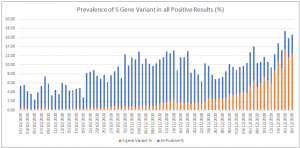
Image courtesy of BBC
The South African strain appears even more infectious than the new UK strain. It came to dominate the country quickly: first found in October, it was responsible for over 80% of all new COVID cases by the end of December.
To corroborate this research, let’s compare new daily COVID cases per million people over the last several months.
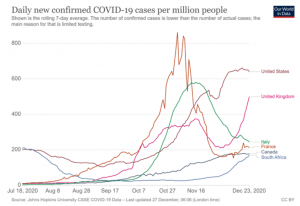
Image courtesy of Our World In Data
The UK, US, Canada, Italy, and France all experienced a major rise in cases in September and October. That’s mainly because colder weather in the Northern Hemisphere drove people to interact indoors, where COVID spreads much more easily.
All these countries imposed various levels of lockdown in late October and early November. That decreased or stabilized their numbers by late November and early December, with the exception of a Thanksgiving-induced bump in the US that stabilized by mid-December.
The UK’s numbers, however, look different. After going from under 250 new cases per day in the start of October, it went to nearly 400 by mid-November. By early December, it successfully bent the curve, with new cases dipping below 250 again. However – unlike any of the other countries – it then experienced a sharp uptick from 250 in early December to over 500 by the end of December. Given the UK didn’t experience any holiday bumps or changes in government policy, the new strain offers a very convincing culprit for this deadly surge.
By contrast, South Africa is in the Southern Hemisphere, and it’s summer there from December to February. So COVID cases should decrease, not increase. However, South Africa experienced a major surge, from below 30 cases per day in early November to over 180 by the end of December. Given no policy changes or other viable explanations, the new COVID variant is almost certainly to blame.
Why We Ignore Slow-Moving Train Wrecks
How worried do you feel right now? Is your heartbeat pounding, do you feel a wave of heat, are your palms sweating? Are you thinking about how to change all your plans for the next six months?
Probably not, because our minds aren’t well adapted to processing the implications of these seemingly-abstract numbers. We fall into dangerous judgment errors that scholars in cognitive neuroscience, psychology, and behavioral economics like myself call cognitive biases. They result from a combination of our evolutionary makeup and also particular ways that our brains are wired.
Such mental blindspots impact all areas of our lives, from health to politics and even shopping. Fortunately, recent research has shown effective and pragmatic strategies to defeat these dangerous judgment errors, starting by learning about those three most likely to harm us in the pandemic.
We suffer from the tendency to focus on the short term, and minimize the importance of longer-term outcomes. Known as hyperbolic discounting, this cognitive bias causes us to underestimate the eventual impacts of clear trends, such as a more infectious strain of COVID.
The normalcy bias results in us feeling that things will generally keep going as they have been — normally. As a result, we underestimate drastically both the likelihood of a serious disruption occurring and the impact of one if it does occur. Indeed, while evaluating the future based on past experience often works, it’s not a good approach for new situations like a novel variant.
When we develop plans, we feel that the future will play out according to these plans. That mental blindspot, the planning fallacy, threatens our ability to prepare effectively for and pivot quickly when facing risks and problems. That includes neglecting both major unknown threats, also known as black swans, as well as, more surprisingly, big and obvious threats, known as gray rhinos; the new strains fall into the latter category.
The Implications of Much Higher Infectiousness
Let’s not make the same mistakes we made in the beginning of the pandemic, making sure to take seriously the real threat of these new strains. So what are the implications?
It took the UK about two weeks to double its numbers from December 10 at 240 new cases per day to December 24 with 506 cases. In South Africa, we see a similar pattern of doubling, from 86 cases on December 10 to 182 on December 24. In both cases it took about two to three months from discovery of the variant to the start of the case surge as the new variant took over.
Given that the new variant was discovered in the US in December and that both variants had likely landed in the US by mid-November, we can anticipate they have started taking over. Based on the examples of the UK and South Africa, they will likely become predominant in March or April. You can expect to see a gradual rise in cases as these strains begin to grow in February and March; then, a sharper surge as they become prevalent in April, doubling every two weeks.
After the post-Thanksgiving bump, the US has maintained a daily new case count of just over 200,000 from December 10 to December 24. What will happen once it starts doubling? Our current rate of just over 200,000 cases per day will be at 400,000 in two weeks. Then, at 800,000 in two more weeks, and then at 1,600,000 in two more weeks.
Imagine what that means. Hospital systems in California, Texas, and other states are already overwhelmed, resulting in rationing care and even turning away patients. What happens if in two weeks, their patient load doubles, then quadruples, and so on? New York City’s terrible outbreak in March will seem like a summer shower compared to the upcoming tsunami that will flood our medical systems.
It’s hard to imagine, but the numbers don’t lie. And of course, hospitals are only part of the picture.
The surge will undoubtedly cause major shortages. That’s due both to supply chain disruptions as employees get sick in large numbers, and also as shoppers engage in panic buying. Industries badly hit by the virus, such as travel and hospitality, will be hammered even more.
Won’t Someone Do Something?
The doubling every two weeks will occur under the current US interventions policies: won’t those with power address the problem?
Perhaps, but it’s unlikely. Given their focus on the effectiveness of vaccines against the new strains, they will most likely emphasize improving vaccine production and distribution, which has already been delayed.
If we get back on schedule, by the end of February, we should finish vaccinating the 24 million in nursing homes and medical staff. We’ll then start on the next phase, the 20 million Americans over 75 not in nursing homes, and the 30 million front-line essential workers, and hopefully will finish by April. But that will be less than a quarter of the over 330 million US citizens. The vaccines will start making a real difference in the summer, especially when Pfizer starts delivering the second batch of 100 million shots in July. We’re facing a very dark Spring.
What about government restrictions, such as the lockdowns recently introduced in the UK and South Africa to battle the strains, or perhaps a ban on foreign nationals to restrict the import of these new strains into the US as announced by Japan? We shouldn’t hope for the latter. The CDC has announced that it will require negative COVID tests from UK travelers. That won’t help with the many people who have COVID but aren’t sick enough to test positive yet.
Politicians won’t impose lockdowns unless they see a clear surge. Unfortunately, we can expect the post-Christmas and New Year infection bumps to hide the impact of the much greater infectiousness of the new strains. Officials will expect numbers to rise in January and then stabilize by February.
When they see numbers keep going up, they will start to express concerns and look for the cause. By the time they home in on the new strains as the source of the problem, and especially by the time they convince top politicians to act, it will of course be too late.
After all, there’s extreme politicization, widespread protests against, and severe economic pain from pandemic restrictions in the US, which were arguably overdone early in the pandemic. Thus, the large majority of governors – those with the true authority over restrictions – feel very reluctant to impose the kind of severe lockdown necessary to fight the new strains.
Even if some do, it’s unlikely that people will follow the restrictions. Consider the case of California. The governor instituted strict restrictions in early December following the Thanksgiving spike. However, pandemic fatigue led to mass public noncompliance, protests, and police officers refusing to enforce the lockdowns.
We can expect the same elsewhere around the country as the new strains take root. Lockdowns won’t be introduced until way too late and protests against lockdowns will sweep the country once again. And while the Biden administration’s intention to issue a mask mandate for federal buildings and request for mass mask wearing will help, it won’t do much.
What Can You Do?
For yourself as a private citizen and your household, change your plans:
- Prepare for months of mass supply chain disruptions by getting non-perishable supplies of consumables, ideally using online sources that won’t empty store shelves for others
- Prepare for lack of access to emergency medical care by minimizing risky activities such as skiing, travel, or substantial household repairs
- Take steps right now to get into strict pandemic lockdown for your household until you all get vaccines: that means avoiding indoor interactions with those outside of your household, or at most brief interactions while masked; wearing masks when outside if you can’t be more than 12 feet away; getting groceries and other essentials delivered instead of going to sores if at all possible; delaying non-emergency medical visits
- To the extent possible, insist on working from home, or invest in a career transition to permit work from home
- Communicate to your friends and family about the new strains and encourage them to take steps to protect themselves until they have vaccines
- Protect the more vulnerable, such as by taking extra precautions around friends and family members over 60 or those with illnesses that make them more vulnerable to COVID such as diabetes
- Be ready to deal with other people making poor decisions, and take whatever steps you need to address such problems
- Prepare psychologically for the tragedy of massive deaths as our hospitals get overwhelmed
If you’re a leader, then prepare your team for this situation:
- Communicate to them about the new strains and encourage them to take the steps above to protect their households
- Strongly encourage your employees to take advantage of any mental health resources you offer to prepare for the trauma of mass deaths
- Coordinate with your HR on how to compensate for the much higher likely caseload of COVID in your team and burnout due to trauma caused by mass deaths and ensure cross-training for key positions
- Transition now to your team working from home as much as possible
- Revisit your business continuity plan to prepare for mass disruptions in the Spring and Summer
- Prepare for major disruptions to your supply chains and service providers, as well as travel disruptions and event cancellations
- By taking all of these steps early, you will have a major competitive advantage, so get ready to use the consequences of this competitive advantage to seize market share from your competitors who fail to prepare
Conclusion
We’re in for a world of pain this Spring and early Summer. It may feel unreal, but that’s simply our cognitive biases telling us that, just like they did early in the pandemic. Don’t be caught off guard, again, by ignoring this warning.
Key Takeaway
We greatly underestimate the dangers of the new COVID strains due to cognitive biases such as normalcy bias, hyperbolic discounting, and planning fallacy. We need to change our plans drastically to adapt to the new reality…> Click to tweet.
Questions to Consider (please share your thoughts in the comments section)
- How alarmed do you feel about the new COVID strains and might you feel insufficiently alarmed due to normalcy bias, hyperbolic discounting, and planning fallacy?
- What might you and your team gain from addressing normalcy bias, hyperbolic discounting, and planning fallacy in your approach to the pandemic and other major disruptors?
- What next steps will you take to change your plans to adapt for the new strains?
Image credit: Wikimedia Commons
Originally Published at Disaster Avoidance Experts on January 5th, 2021


